Cogan’s Occulomotor
Apraxia, dyspraxia, dyslexia, binocular instability... a case study
Abstract
A study of
visual intervention, to improve reading performance (phonological processing) of a young man originally
identified having congenital occulomotor apraxia (COA).COA interferes with
visual search mechanisms by restricting the formation of saccadic eye movement,
He was then identified as being Dyspraxic and later as he entered Higher
education he was assessed for dyslexia and was identified as dyslexic.
This
intervention took about 1 hour and application of the findings appears to give
rise to a measurable increase in phonological processing speed of 21%...
The testing
included recording and measurement of his eye movements, which are subliminal
at different stages.
The control of
saccades and fixations are managed by the cerebellum in response to visual
processing data and in turn feedback to the edge detection data which is a
product of the controlled saccades and fixations. This can be considered in the
context of the work on the relationship between cerebellum functioning and
dyslexia as centred in the UK at the University of Sheffield led by Nicholson
and Fawcett. It can also be considered in the context of the ideas on
magnocellular deficit and dyslexia developed in UK by John Stein et al at Oxford
with its ideas on binocular instability which is considered to be dependent on
cerebellar function.
This week I had the privilege of working with a
young man (‘A’ )who was diagnosed in his first year of life as having ‘Cogan’s occulomotor
apraxia’ ( Google it for more information).
This is a condition which is congenital and is
linked with the initiation of saccades; the rapid eye movements which redirect
the eyes to new objects of attention. In the graphs on eye movement in previous
blogs these are the vertical lines on the graph as the eyes move from one word
to the next...Or the end of one line to the beginning of the next line.
It is not that the eyes cannot do these movements;
it is that there appears to be a fault in the mechanism which means that they
sometimes do and sometimes do not occur.
When using a binocular eyetracker with many
dyslexic adults, it is quite common for one of the eyes not to saccade when reading in a
default computer screen environment.
When A was young he was diagnosed as being Dyspraxic, which is defined below.
Developmental dyspraxia is an impairment or
immaturity of the organisation of movement. It is an immaturity in the way that
the brain processes information, which results in messages not being properly
or fully transmitted. The term dyspraxia comes from the word praxis, which
means 'doing, acting'. Dyspraxia affects the planning of what to do and how to
do it. It is associated with problems of perception, language and thought.
A typically broad definition, but it was the origin, in a
way, of a great deal of research into Dyslexia
at Sheffield University. Rod
Nicholson and Angela Fawcett’s work showed a statistical relationship between
muscle tone management and the reading difficulties associated with Dyslexia.
This led to intervention work concerned with attempts to train the Cerebellum, which is the brain’s centre for
muscle tone management and coordination.
At one extreme it led to the throwing bean bags in the air, wobble
boards, to try and remediate ‘the problem’.
It also led to the overlap in the protocols for the identification of people
with dyslexia and dyspraxia and much confusion.
Children with COA need a proactive interaction to
mitigate the effects, such as speech therapy and hand eye coordination
excercises. There are strategies which the person develops to initiate
saccades, such as head thrust. Brief sideways jerking of the head) As such with
appropriate support the effects of the apraxia become less and less disabling
as the person goes through their second and third decade.
In the case of A, a remaining issue is his dyslexic
characteristic. My task was to investigate what was really happening visually
and to find out if his reading performance (phonological processing output!)
could be improved by adjusting the
visual processing input.
Stage
1
Is
there any history of ophthalmic problems?
Visits to opticians suggest that there are no focussing problems
that can be dealt with by ophthalmic intervention. .. Vision is normal. A relatively quick check by myself confirmed
this to be the case.
His job is that of a graphic artist. Precise vision is
needed for this. An example of his work is
given below. (Google Jakgibberish for more examples)

Stage
2.
Find
out about his eye movement management in non reading activities.
The graph below shows A’s eye movements during normal
visual activity; looking around the room we were sitting in...

Normally you would expect the two eye traces to be
matched with distinct, synchronised saccades and fixations. The left eye (the red line) does show a few
saccades, I can pick out six by the right eye (blue line). There are no clear
fixations by the right eye and the right eye goes into a nystagmus occasionally
which interrupts the work of the left eye, pulling it sideways.
Head movements would show up as a sloping
graph, but if both eyes were ‘linked together normally the angle of the slope
would be the same for both eyes. This is not happening here.
Stage
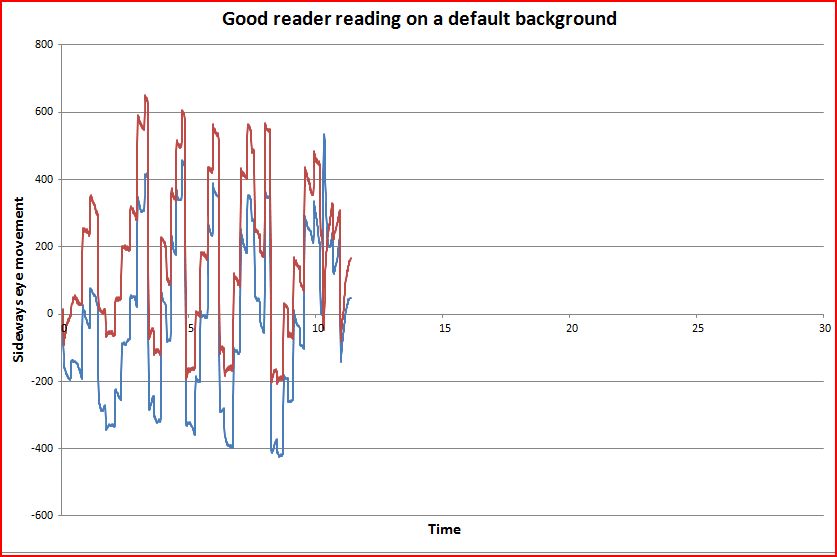
3... Finding out what happens in default reading conditions, the default is a
default (12) font with a white background.

A’s left eye, is moving in a rational way typical of many
readers with clear saccades and fixations, but with many regressions . His
right eye meanwhile, has been turned in towards his nose (to the left) and is
no longer looking towards the text. For his right eye there are no clear
saccades except at the ends of lines.
The rest of the time, the movements of his ‘reading left
eye’ are not influencing/ controlling his right eye. Although in the third and
fourth line, the gradual upward movement during each line suggests that there
is some linkage. You can see three
bursts of nystagmus type activity as well.
We can conclude here that there is no initiation of
saccades, no ‘visual search’, no attention originating, fixations associated
with the right eye, which is a functioning eye.
A decision has been made by his visual system to suppress it! In
biological terms this implies that he is getting better visual data, by using visual
data from only one eye; his left onewhatever the visual activity.
Stage
4. Get a measurement of reading performance.
Using the same Oral reading fluency test that has been
used with over 12,000 adults, A read off a computer screen with a font 12 and
‘white background’
Default Oral reading fluency…….105 wpm
The reading style was stocatal; individual words were
being read in syllables; limited blending.
The mean reading speed for this text by dyslexic
undergraduates is 138 wpm. For non dyslexic undergraduates it is 184 wpm. I can quote Standard deviations but not here.
At the conclusion we will measure Oral reading fluency (a
measure of phonological processing) with an equivalent text, using whatever
optimal settings we identify.
Stage
5..Find out if font size influences reading performance.
This was
undertaken binocularly. The data was unclear. There was a hint that a larger
font than default 12 might be useful and it was decided to use
font 16 point for the next stage.
For
many dyslexic people there is a clear mathematical relationship between font
size and reading performance. See the other posts on this blog.
At this point it became clear that testing A binocularly
was going to be too stressful. The
screen optimisation continued monocularly using only his ‘good’ left eye.
His right eye was covered. This meant that it would still move dependent only
on visual data collected by his left eye,
Stage
6... Find out if screen brightness influenced reading performance.

There was a linear relationship between screen brightness
and reading performance. Reduction of overall brightness gives rise to a slower
reading output.
For
the majority of dyslexic undergraduates the screen brightness needs to be
reduced.
Stage
5. Finding out if reading performance was affected by red or green pixel
brightness.
A
did respond to changing the green pixel brightness but it was a far smaller
effect.
Stage
6...Response of reading performance to Blue pixel brightness
There was no response
to changing the blue pixel brightness... The magnocellular difference model of developmental
dyslexia implies that a response would be expected. But there was none.
Actually
very few dyslexic undergraduate respond significantly to changes in blue pixel
brightness.
Stage
7...Checking Oral reading performance with the identified screen settings.
This was using a font 16 and the following background screen settings.

Oral
reading performance…..127 wpm.
In addition the reading ‘style’ was more fluent, whole
word enunciation now being with a clearly prosodic component.
This is a 21% measurable increase in
performance.
I
have not yet found a way to quantify Prosodic performance, but I am following
the development of The PRAAT methodology in this area. (Please google this if
you are interested.)
Stage
8... Finding out how A’s eyes were behaving in the new conditions.

This was not quite what I expected. But in retrospect his right eye had been
covered virtually continuously for about 30 minutes! By the end of reading the
text both eyes were starting to work together, this can be seen especially in
the third and fourth line. But there
are still the quite distinctive nystagmus zones when the trigger mechanism is
breaking down.
A series of readings were then done reading monocularly.
From previous experience A was asked to read for a while using only his right eye and the optimal conditions. This is
an attempt to get the ‘brain’used to a new capability.
Left
eye covered, using only his right (Poor?) eye.

The interesting thing here is that with the optimal
background and with no data coming into his left eye, the data being collected
by the right eye was able to enable the control of the movement of his left eye
.
Right
eye covered, using only his left eye.
With his right eye covered, the data being collected by
the left eye, His right eye moved in time with the controlling left eye, although
it did not show the crispest saccades and fixations But the fixation disparity (distance
between the attention points) of the two eyes was more erratic than when it was
the right controlling the left.

Finally
an eyetrace was undertaken binocularly with a small font (10 point) such that
more data was landing in the foveal area of the retina...

The two eyes are now yoked together, but the font
probably too small for the highest quality of fixation.
The graph below shows detail over a 2 second period,
which is typical of the entire graph above. Both eyes show clear yoked saccades
and fixations, but the right eye shows slight fixation instability. But this is
typical of many good readers.

The slight right eye fixation instability most likely would be
solved with a slightly larger font.
We will now wait for a while for A to make use of his
settings in reading/inputting computer activity during which time it is likely (I
think) that there will be a change in the innervations (how many motor end
plates are used in the muscle fibres) and control of the core muscle fibres In
the occulomotor muscles of his right eye, which are responsible for managing
the actual fixations. (This is a new experience for his eye muscles!)
If you are interested in histology and muscle fibre
design I commend you to look at them literature ion this area. Occulomotor muscles are I believe their own
class. They are not cardiac, smooth or skeletal in design. They have a
fascinating histology and physiology of their own; befitting their role in
precise strategic visual data collection.
Wait
for the next thrilling instalment in the control of phonological output by the
visual processing system!
I
look forward to comments and questions.